[fullwidth background_color=”#ebebeb” background_image=”” background_parallax=”none” enable_mobile=”no” parallax_speed=”0.3″ background_repeat=”no-repeat” background_position=”left top” video_url=”” video_aspect_ratio=”16:9″ video_webm=”” video_mp4=”” video_ogv=”” video_preview_image=”” overlay_color=”” overlay_opacity=”0.5″ video_mute=”yes” video_loop=”yes” fade=”no” border_size=”0px” border_color=”” border_style=”solid” padding_top=”0″ padding_bottom=”0″ padding_left=”” padding_right=”” hundred_percent=”yes” equal_height_columns=”no” hide_on_mobile=”no” menu_anchor=”” class=”” id=””][imageframe lightbox=”no” lightbox_image=”” style_type=”none” hover_type=”none” bordercolor=”” bordersize=”0px” borderradius=”0″ stylecolor=”” align=”center” link=”” linktarget=”_self” animation_type=”0″ animation_direction=”down” animation_speed=”0.1″ hide_on_mobile=”no” class=”” id=””]  [/imageframe][/fullwidth][fullwidth background_color=”#ffffff” background_image=”” background_parallax=”none” enable_mobile=”no” parallax_speed=”0.3″ background_repeat=”no-repeat” background_position=”left top” video_url=”” video_aspect_ratio=”16:9″ video_webm=”” video_mp4=”” video_ogv=”” video_preview_image=”” overlay_color=”” overlay_opacity=”0.5″ video_mute=”yes” video_loop=”yes” fade=”no” border_size=”0px” border_color=”” border_style=”solid” padding_top=”40″ padding_bottom=”40″ padding_left=”” padding_right=”” hundred_percent=”no” equal_height_columns=”no” hide_on_mobile=”no” menu_anchor=”” class=”” id=””][two_third last=”no” spacing=”yes” center_content=”no” hide_on_mobile=”no” background_color=”” background_image=”” background_repeat=”no-repeat” background_position=”left top” border_position=”all” border_size=”0px” border_color=”” border_style=”” padding=”” margin_top=”” margin_bottom=”” animation_type=”” animation_direction=”” animation_speed=”0.1″ class=”” id=””][fusion_text]
[/imageframe][/fullwidth][fullwidth background_color=”#ffffff” background_image=”” background_parallax=”none” enable_mobile=”no” parallax_speed=”0.3″ background_repeat=”no-repeat” background_position=”left top” video_url=”” video_aspect_ratio=”16:9″ video_webm=”” video_mp4=”” video_ogv=”” video_preview_image=”” overlay_color=”” overlay_opacity=”0.5″ video_mute=”yes” video_loop=”yes” fade=”no” border_size=”0px” border_color=”” border_style=”solid” padding_top=”40″ padding_bottom=”40″ padding_left=”” padding_right=”” hundred_percent=”no” equal_height_columns=”no” hide_on_mobile=”no” menu_anchor=”” class=”” id=””][two_third last=”no” spacing=”yes” center_content=”no” hide_on_mobile=”no” background_color=”” background_image=”” background_repeat=”no-repeat” background_position=”left top” border_position=”all” border_size=”0px” border_color=”” border_style=”” padding=”” margin_top=”” margin_bottom=”” animation_type=”” animation_direction=”” animation_speed=”0.1″ class=”” id=””][fusion_text]
Peripheral Nerve Surgery
Problems with peripheral nerves requiring surgery may come under the care of neurosurgeons.
Included amongst these are traumatic lesions (peripheral nerves in the limbs, brachial plexus injuries, maxillary nerve avulsions), compressive lesions (carpal tunnel syndrome, ulnar neuropathy, lateral popliteal nerve palsy, meralgia paraesthetica) and lesions involving tumours affecting peripheral nerves (neurofibromas, Schwannomas).
Many of these are also treated by other disciplines (plastic surgeons, hand surgeons, general surgeons, orthopaedic surgeons), but few cover the full spectrum.
Carpal tunnel syndrome
The commonest compression neuropathy, carpal tunnel syndrome typically presents with recurrent sensory disturbance (numbness, pins and needles), pain and, in advanced cases, muscle weakness, affecting one or sometimes both hands.
The sensory disturbance is in the distribution of the median nerve (thumb, index and middle fingers), but often it feels “like the whole hand”.
Typically nocturnal symptoms are prominent, sometimes waking the patient several times each night.
Confirmation of the clinical diagnosis is by nerve conduction studies, performed by a neurologist.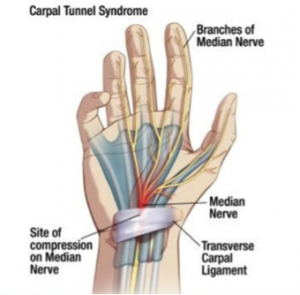
Some cases are associated with disease states (acromegaly, hypothyroidism), some with physiological conditions (pregnancy), and some with recurrent stress patterns (certain repetitive activities or occupations), but most are related to age linked changes, causing narrowing of the space beneath the transverse carpal ligament at the wrist through which pass the flexor tendons to the fingers and the median nerve.
It is compression of the median nerve that produces the symptoms.
Treatment options include activity modification, splinting, steroid injection and decompressive surgery if no underlying disease requires attention. Surgery is usually very effective in resolving the symptoms, and protects the nerve against further deterioration. It is indicated if non-surgical treatments fail to adequately control symptoms, and particularly if the nerve conduction studies indicate severe electrophysiological changes.
Ulnar neuropathy
Problems with the ulnar nerve most commonly arise at the elbow but occasionally at the wrist
 The ulnar nerve is vital in controlling the muscles responsible for fine motor control in the hands, and its impaired performance can result in loss of dexterity and significant impairment.
The ulnar nerve is vital in controlling the muscles responsible for fine motor control in the hands, and its impaired performance can result in loss of dexterity and significant impairment.
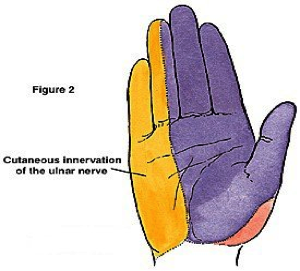
Its sensory distribution is to the little finger border of the hand, the little finger, and half the ring finger.
Problems at the elbow may occur in relation to chronic trauma, or deformity, but are most commonly associated with thickening and fibrosis of the margins of the ulnar groove, or below that in the cubital tunnel where the nerve enters the forearm. At the wrist, the nerve is vulnerable to repeated trauma, or extrinsic compression, often by a ganglion arising from the nearby wrist joints.
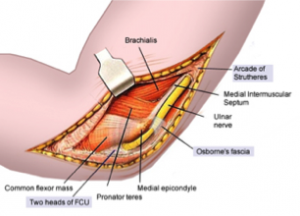 Treatment may involve activity modification, but may require direct intervention to decompress the affected part of the nerve, particularly if the changes on nerve conduction testing are severe. If elbow deformity is present, consideration may be given to transposing the nerve to lie in a position in front of the medial epicondyle (and thus anterior to the axis of the elbow joint).
Treatment may involve activity modification, but may require direct intervention to decompress the affected part of the nerve, particularly if the changes on nerve conduction testing are severe. If elbow deformity is present, consideration may be given to transposing the nerve to lie in a position in front of the medial epicondyle (and thus anterior to the axis of the elbow joint).
Avoiding delayed treatment is important to prevent the development of a permanently impaired hand.
Lateral popliteal nerve palsy
Dysfunction of the lateral popliteal (common peroneal) nerve leads to sensory change over the lateral calf, dorsum of the foot and great toe, and weakness of the muscles that bend up the ankle in its severe form. This produces a ‘footdrop’, where the ankle does not bend up properly, the toe tends to skuff the ground, and the gait is altered to accommodate (‘high stepping’).
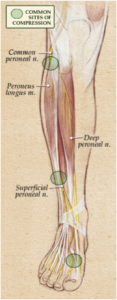 The nerve lies relatively superficially just below the outside of the knee, on the fibula bone, and it is vulnerable to pressure injury at that point. The classical injury in years past was pressure from a plaster cast for a fracture below the knee.
The nerve lies relatively superficially just below the outside of the knee, on the fibula bone, and it is vulnerable to pressure injury at that point. The classical injury in years past was pressure from a plaster cast for a fracture below the knee.
Nerve conduction studies are useful to confirm the diagnosis, and to help differentiate the cause from a nerve root compression problem in the lower back.
If recovery does not occur after relief of any external compression, exploration of the nerve may be required to decompress internally from fibrosis or, occasionally, from compression by a ganglion arising out of the tibio-fibular joint.[/fusion_text][/two_third][one_third last=”yes” spacing=”yes” center_content=”no” hide_on_mobile=”no” background_color=”#f7f7f7″ background_image=”” background_repeat=”no-repeat” background_position=”left top” border_position=”all” border_size=”0px” border_color=”” border_style=”solid” padding=”20px” margin_top=”” margin_bottom=”” animation_type=”0″ animation_direction=”down” animation_speed=”0.1″ class=”” id=””][fusion_widget_area name=”avada-custom-sidebar-otherneurosurgicalconditions” background_color=”#f7f7f7″ padding=”10px” class=”” id=””][/fusion_widget_area][/one_third][/fullwidth]